Immunohistochemical results are particularly important for the diagnosis, treatment and prognosis of lung cancer.
I. lung adenocarcinoma
1、TTF-1
TTF-1 (thyroid transcription factor-1) is expressed in the nuclei of thyroid follicular and alveolar epithelial cells. It is positively correlated with the degree of tumor differentiation. The worse the differentiation is, the more likely the expression is missing.
About 75% - 85% of lung adenocarcinoma expressed positive. Squamous cell carcinoma usually does not express TTF-1 (so TTF-1 is mainly used to distinguish adenocarcinoma and squamous cell carcinoma, and cannot distinguish lung adenocarcinoma and nets).
TTF-1 is expressed in pulmonary neuroendocrine tumors (NETs), including carcinoid (typical carcinoid TC, atypical carcinoid AC), 50% of large cell neuroendocrine carcinoma (LCNEC) and 90% of small cell lung cancer (SCLC)
TTF-1 is almost negative in metastatic adenocarcinoma of the lung, which is differentiated from thyroid tumor: TG is negative;
In addition, TTF-1 was found to be expressed in a small number of ovaries (3% - 39%), endometrium (2% - 23%) and cervical adenocarcinoma (4%).
2、CK7(cytokeratin-7)
Almost 100% of lung adenocarcinoma express CK7, but the specificity of CK7 is low, and 30% - 60% of lung squamous cell carcinoma are positive. It can also be expressed in adenocarcinoma of breast, stomach, ovary, pancreas, uterus, urothelium and other organs and parts.
The differential diagnosis of lung adenocarcinoma should be combined with TTF-1 and Napsin a.
3、Napsin A
Napsina (New aspartate protease A) is expressed in normal alveolar type II epithelial cells and proximal and distal renal tubules, and more than 80% is expressed in lung adenocarcinoma. Its sensitivity and specificity are better than TTF-1.
Similar to TTF-1, the expression of Napsin a in lung adenocarcinoma is also correlated with histological type and degree of differentiation.
3% of lung squamous cell carcinomas express Napsin a, while lung neuroendocrine tumors do not express Napsin a (which can be used to differentiate between lung adenocarcinoma and nets). It can also be expressed in some metastatic lung cancer, such as renal cell carcinoma, a small number of thyroid papillary carcinoma, endometrial adenocarcinoma, ovarian adenocarcinoma, cholangiocarcinoma, etc.
TTF-1 and Napsin a are currently one of the best antibody combinations for the diagnosis of lung adenocarcinoma.
2、 Squamous cell carcinoma of lung
1、p63
More than 90% of lung squamous cell carcinomas have strong positive nuclei, but 10% - 33% of lung adenocarcinoma have focal low-level expression of p63.
P63 was also expressed in 15% of neuroendocrine cancers and 22% of small cell lung cancer.
2、p40
P40 is one of the subtypes of p63 protein, and its positive location is in the nucleus. It is considered to be the most specific and sensitive marker of squamous cell carcinoma.
Its sensitivity is similar to p63, but its specificity is better than p63. More than 96.8% of squamous cell carcinoma is positive, and adenocarcinoma is basically not expressed (3-5%), and it is often expressed locally. Among endocrine tumors, carcinoid did not express, 3.6% in large cell lung cancer and 2.4% in mesothelioma.
3、CK5/6
Ck5/6 is normally expressed in squamous epithelial cells, basal cells of ductal epithelium, myoepithelial cells and mesothelial cells.
75%~100% of lung squamous cell carcinoma has expression, and it has nothing to do with differentiation and grade. 2% to 33% of lung adenocarcinoma can express ck5/6, but it often shows focal low-level expression. 75% - 100% of pleural epithelioid malignant mesothelioma also expressed.
4、DSG3
Dsg3 (desmosomes core glycoprotein) is expressed in 85% - 90% of lung squamous cell carcinoma, and almost not in lung adenocarcinoma (<2%).
92.6% of squamous cell carcinoma can be diagnosed by ck5/6 and Dsg3 85% of lung adenocarcinoma and squamous cell carcinoma can be distinguished by Dsg3 and Napsin a.
3、 Neuroendocrine tumor
1、Syn
Syn (synaptophysin) mainly exists in the presynaptic vesicle membrane of neurons, adrenal medulla, carotid body, and neuroendocrine and epithelial neuroendocrine cells of skin and viscera.
This antibody is mainly used to label neuroendocrine cells and their tumors.
2、CgA
CGA (chromaffin a) is a soluble acidic protein with the highest content in human adrenal medulla. It widely exists in neurons, neuroendocrine cells and tumor cells.
It is mainly used to mark neuroendocrine tumors, such as pituitary tumors, islet cell tumors, pheochromocytoma, medullary thyroid carcinoma, carcinoid, etc.
3、CD56
Neural cell adhesion molecules (NCAM, CD56) are expressed in NK cells, a small number of activated T lymphocytes and cells of neural ectodermal origin.
This antibody is a marker of NK cell lymphoma and the preferred specific marker of pulmonary neuroendocrine tumors.
4、Ki-67
Ki-67 is a nuclear antigen related to cell proliferation, and its function is closely related to mitosis. Ki-67 marks cells in the proliferation cycle. The higher the positive rate is, the faster the tumor grows, the worse the tissue differentiation is, and the more sensitive it is to chemotherapy.
Ki-67 has dual effects on the diagnosis and grading of pulmonary neuroendocrine carcinoma. For example, the Ki-67 proliferation index of typical carcinoid is ≤ 5%, which belongs to low level, the atypical carcinoid is 5% - 20%, which belongs to medium level, and the large cell lung cancer is usually ≥ 60%, which belongs to high level.
4、 Differentiation between adenocarcinoma and squamous cell carcinoma of the lung
TTF-1, Napsin a, ck5/6 and p63 (P40) are the most commonly used antibody combinations to distinguish lung adenocarcinoma and squamous cell carcinoma.
Generally, ttf-1/p63 combination is positive and negative in both adenocarcinoma and squamous cell carcinoma.
• if ttf-1/p63 are both positive, we tend to diagnose adenocarcinoma, because p63 can be expressed in adenocarcinoma, while TTF-1 is rarely diffusely expressed in squamous cell carcinoma (> 50% of tumor cells).
• if ttf-1/p63 are all negative, adenocarcinoma is still suspected, because the lack of expression of TTF-1 in poorly differentiated adenocarcinoma is common, while the expression of p63 in squamous cell carcinoma is very stable.
All squamous cell carcinoma markers could not distinguish metastatic squamous cell carcinoma, epithelial carcinoma, and even sarcoma and large cell lymphodynia (p63 could be positive). P40 is not expressed in the above-mentioned large cell lymphoma, so choosing P40 instead of p63 can effectively avoid misdiagnosis of lung or mediastinal large cell lymphoma as squamous cell carcinoma.
5、 Differentiation between primary and secondary lung tumors
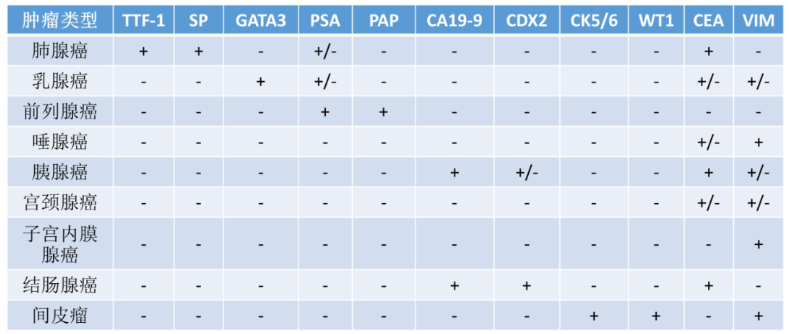
Generally speaking, adenocarcinoma that metastasizes to the lung is common in breast cancer, pancreatic cancer, prostate cancer, cervical adenocarcinoma, endometrial cancer, colon adenocarcinoma and mesothelioma. Usually, metastatic tumors and primary tumors share the same antigen expression.
6、 Differentiation between lung cancer and pleural mesothelioma
There are no 100% specific markers, so at least 2 mesothelial and 2 epithelial markers should be selected.
According to the sensitivity and specificity of antibodies, the best markers of mesothelioma are calretinin, CK5 or ck5/6, Wilms tumor gene 1 (WT-1) and D2-40.
7、 Differentiation of large cell lung cancer
According to the definition (who2015), large cell lung cancer is an undifferentiated non-small cell lung cancer, which lacks the characteristics of small cell carcinoma, adenocarcinoma and squamous cell carcinoma in cytology, histological structure and immunophenotype, and it must be surgically removed specimens to make the diagnosis of large cell carcinoma. Immunohistochemistry and mucus staining are necessary for the diagnosis of large cell carcinoma.
Reference links: