The damage of chemotherapy drugs to the nervous system is called "peripheral neurotoxicity after chemotherapy (CIPN)". It is common to have symmetrical pain, numbness and tactile abnormalities in the distal extremities. In severe cases, it may involve the proximal extremities, accompanied by disappearance of tendon reflex or dyskinesia.
CIPN mostly belongs to dose limiting toxicity. With the continuous accumulation of the dose of chemotherapy drugs, the symptoms will be aggravated, and even cause permanent nerve damage.
According to the impact of peripheral neurotoxicity on people, the National Cancer Institute (NCI) divides it into the following levels:
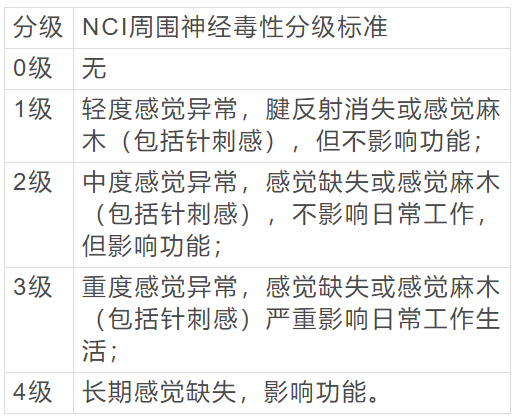
Note: tendon reflex refers to involuntary muscle contraction during rapid tendon traction.
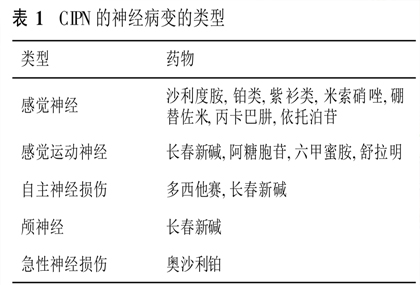
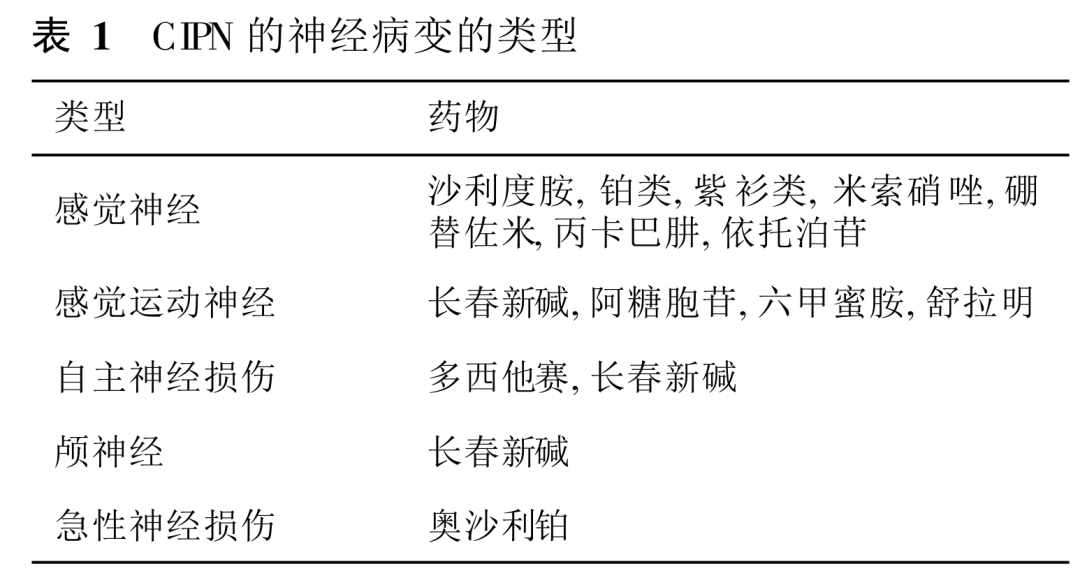
Neuropathy types of CIPN
Common chemotherapy drugs that cause CIPN
1. Oxaliplatin
Oxaliplatin induced neuropathy is very common in clinic. Compared with other forms of peripheral neurotoxicity, oxaliplatin induced neurotoxicity has unique clinical symptoms and signs. There are two different clinical manifestations:
• acute toxicity: acute symptoms can occur more than a few hours after infusion of the drug. About 85% - 95% of patients have temporary sensory disorders within a few hours or days after treatment, manifested as numbness and pain in the distal limb, sometimes numbness in the mouth and lips, and obvious aggravation in cold, which can be relieved by themselves.
• chronic toxicity: the chronic symptoms are mainly due to the accumulation of red blood cells combined with platinum, which is manifested in the sensory dullness and abnormal sensation of the extremities, and even the spasm of the upper respiratory tract and upper gastrointestinal tract, and acute pharyngeal spasm. When the cumulative dose is greater than 800mg/m2 (about 8-10 cycles), the probability of dysfunction is higher. About 16% - 21% of patients are affected by this in their daily life, but it is usually reversible. They can continue to take medicine after a proper rest.
2. Cisplatin
Cisplatin is generally useless drugs with early neurotoxicity, and its neurotoxicity is positively correlated with the cumulative dose. When the cumulative dose of cisplatin in adults reaches 400-700mg/m2, there will be sensory abnormalities, early manifestations are painful sensory abnormalities and numbness. With the increase of the cumulative dose, there will be vibration loss, ataxia, and even sensory loss. Generally, the damage is reversible 3-6 months after withdrawal.
3. Vinblastine
Vinblastine includes vincristine, vinoresin, vinblastine and vinorelbine. Neurotoxicity is the main adverse reaction of vinblastine, which is dose limiting toxicity.
The neurotoxicity of vincristine, vinoresin and vinblastine is characterized by numbness, pain and weakness in the limbs, dull or even disappearance of tendon reflex, paralytic intestinal obstruction and cerebral nerve paralysis, which last for a long time.
The neurotoxicity of vindesin is 1/2 that of vincristine, and the neurotoxicity of vinblastine is more obvious, which generally occurs within 3 months before treatment.
Vinorelbine has a higher incidence of neurotoxicity in similar drugs because it has more affinity for mitotic microtubules. After long-term medication, it can cause lower limb weakness, constipation caused by small intestinal paralysis, and paralytic intestinal obstruction is rare.
Clinical trials of vincristine liposomes have also confirmed that its toxic reactions are mainly manifested in neuropathic pain and limb numbness, and neurotoxicity is still the main dose limiting factor.
4. Taxus
The main neurotoxicity of Taxus drugs is peripheral, and the incidence of peripheral neurotoxicity is 52%. Most of them occur within 48 hours after administration. The most common is peripheral neuropathy involving sensory nerve fibers, which is characterized by mild limb numbness, paresthesia, and muscle pain. It mainly occurs at the end of the limbs, which is called the "glove / sock" distribution pattern. In addition, optic nerve disorders can occur, characterized by flashing dark spots, The vast majority of patients' symptoms gradually relieved and disappeared after drug withdrawal.
High dose, high cumulative diabetes and previous underlying neuropathy are the risk factors of paclitaxel induced neurotoxicity.
Paclitaxel can also cause other neurotoxic reactions, such as autonomic neuropathy, joint and muscle pain, convulsions and transient encephalopathy. However, paclitaxel can also cause severe acute encephalopathy at extremely high doses (>600m/m2).
The neurotoxicity of docetaxel is similar to that of paclitaxel, but the incidence of hand foot acupuncture sensation and finger and toe numbness is lower than that of paclitaxel, and the neurotoxicity is proportional to its cumulative dose.
Liposome paclitaxel has chosen a special drug carrier, and its systemic toxic and side effects are smaller than paclitaxel, but the incidence of side effects of transient sensory neurotoxicity of liposome paclitaxel is higher than paclitaxel.
5. Thalidomide
Peripheral neurotoxicity is one of the most serious side effects of thalidomide. The anti-tumor and neurotoxicity mechanism of thalidomide is not clear, which may be related to immune regulation, cytokine regulation and inhibition of angiogenesis. Preliminary clinical trials have confirmed that thalidomide analogue lenalidomide has stronger antitumor efficacy and lower incidence and severity of neurotoxicity.
Prevention and treatment of CIPN
The treatment of peripheral nerve damage is still a big problem at present. There are many related drugs, but most of these drugs have poor effects. Therefore, neurotoxicity emphasizes general prevention and nursing measures.
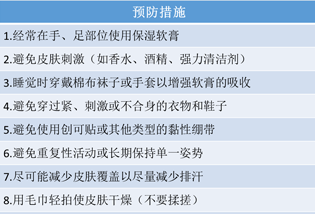
General prevention and treatment measures include:
• ask patients to keep their hands and feet warm, use warm hands and gloves more often, and avoid contact with cold water, cold air and metal objects;
• light diet, avoid spicy and irritating food;
• try not to apply irritant liquids (such as alcohol, soapy water, etc.), ointments (such as sulfur ointment), and reduce the friction of the skin of limbs;
• avoid infusion of chemotherapy drugs from the great veins of the limbs, and try to infusion from the central vein;
• prolonged intravenous administration;
• if peripheral nerve damage occurs, measures such as prolonging the chemotherapy time, reducing the drug dose and stopping the drug can be selected according to the severity of the damage, and the original chemotherapy regimen can be restored after symptomatic treatment.
In addition to general measures, the prevention and treatment of drugs are also very important, including:
1) Ion channel regulators and antiepileptic drugs: including calcium magnesium mixture, pregabalin, gabapentin, and carbamazepine. Pregabalin is commonly used in the treatment of peripheral neuralgia and epilepsy, and calcium magnesium mixture is commonly used in the prevention and treatment of oxaliplatin induced neurotoxicity.
Calcium ion can promote the closure of sodium ion channel by changing the voltage dependent sodium ion channel, and magnesium ion can facilitate the operation of sodium pump by restoring ATP function. In addition, it is found that magnesium sulfate can inhibit nerve fiber stress and has a significant effect on preventing thalidomide related neurotoxicity.
2) Neurotrophic agent: nerve cells have a certain repair ability, and providing sufficient metabolic and repair raw materials is of great significance to promote the repair of nerve cells, and is conducive to the prevention and treatment of neurotoxicity caused by chemotherapy. Its representative drug is Mecobalamin.
Mecobalamin is an active metabolite of vitamin B12 in the body, which can promote the formation of lecithin, promote the formation of medullary cavity of neurons, and stimulate axonal regeneration. Mecobalamin can increase the metabolic activity of neurotransmitters such as acetylcholine, restore the reduced neurotransmitters, and improve nerve tissue transmission and metabolic disorders. Recent experiments have shown that Mecobalamin Combined with reduced glutathione injection has a certain effect on peripheral neurotoxicity.
Other neurotrophic agents such as gangliosides can significantly reduce the incidence of oxaliplatin induced neuropathy, especially severe neuropathy, and do not affect the efficacy of chemotherapy.
3) Antioxidants: the formation of acute peripheral neuropathy may be related to the oxidative damage of nerve cells caused by the induction of superoxide anion production, lipid peroxidation, protein hydroxylation, DNA oxidation, etc., so the use of reductants can antagonize the neurotoxicity of chemotherapy to a certain extent.
Vitamin E and reduced glutathione are internationally recognized anti oxygen free radical drugs. Reduced glutathione is a peptide naturally synthesized by human cells and a neuromodulator. It can combine with free radicals in the body and convert into acids that are easy to metabolize, thereby accelerating the excretion of free radicals. At the same time, it can inhibit the accumulation of drugs in the neurons of the heel ganglion, accelerate the cleaning of drugs, strengthen the functional recovery of nerve cells, and reduce the neurotoxic reaction of drugs.
Amifostine has strong free radical scavenging and antioxidant effects, can loosen the DNA super helix structure, and can also combine with chemotherapy drugs to form a complex to prevent the formation of DNA adducts of chemotherapy drugs. It can combine with DNA nucleoprotein to change the structure of chromatin nucleosomes so that it is not easy to be degraded, so as to reduce the apoptosis of normal tissues caused by chemotherapy drugs. In addition, amifostine can accelerate the repair of defective DNA, It can promote the growth and repair of neuronal axon damage caused by anti chemotherapy drugs, so it has a significant effect on chemotherapy peripheral neuropathy.
4) Tricyclic antidepressants: including duloxetine, norepinephrine and amitriptyline. Duloxetine is currently the only clinically recognized drug that can improve neuralgia caused by peripheral neurotoxicity.
5) Traditional Chinese medicine treatment: at present, a number of clinical studies have confirmed that traditional Chinese medicine has a significant effect on peripheral neurotoxicity caused by chemotherapy drugs. Commonly used prescriptions of traditional Chinese medicine include Buyang Huanwu Decoction, Wenjing decoction, Huangqi Guizhi Wuwu decoction, etc. The use of traditional Chinese medicine for warming meridians and dispersing cold, activating blood circulation and dredging collaterals for medicine bath or external washing also has a certain effect. Local warm acupuncture or moxibustion can warm the meridians and dissipate cold, dredge meridians and activate collaterals, replenish qi and activate blood circulation, and also obtain satisfactory effects on peripheral neurotoxicity after chemotherapy.
In a word, the treatment of peripheral neurotoxicity caused by chemotherapy has limited effect. Paying attention to prevention and reducing the occurrence of peripheral neurotoxicity is the key.
Source link: