Targeted treatment of drug resistance, again genetic testing is the main choice. At this time, the more common question is: do you need to stop the drug before genetic testing? Note that the premise of this problem is that under the condition of clear drug resistance, that is, under the four typical conditions of primary lesion progression (increase by more than 20%), metastatic lesion progression (increase by more than 20%), newly confirmed metastatic lesions, and comprehensive outbreak progression, when the treatment plan needs to be adjusted, the adjustment of targeted therapy should be guided according to the results of new genetic testing to find targeted solutions. That is to say, it is necessary to first identify what causes drug resistance - some of these causes of drug resistance are that new mutations or targets can be found through genetic testing, so as to arrange the subsequent targeted treatment drug change or combination drug regimen, in order to obtain a high effective rate.
In the previous article, we explained the main causes of drug resistance, but considering the progress type of targeted therapy and the specific causes of drug resistance, we deduced and considered the problem of sample selection, the impact of drug withdrawal on what, and finally considered the technical problems of drug withdrawal and gene testing in each case. Each step needs to consider a long chain of basic knowledge and logical demonstration process. In order to facilitate friends who only want to obtain the processing methods and do not want to conduct in-depth research to obtain the maximum reading value from this article, let's directly say the conclusion first.
The gene test after the secondary drug resistance of targeted therapy is to find the cause of drug resistance, not to re verify the original driver gene. Therefore, even if we are forced to use peripheral blood as the gene test sample, we do not need to stop the targeted drug for gene test; If it is a tissue test, it is OK to consider whether to stop the drug according to the side effects of the drug. Here, it mainly refers to bone marrow suppression, severe rash, bleeding tendency and other side effects that may become biopsy interference.
In addition, targeted treatment of primary drug resistance, that is, it is ineffective at the beginning. This is a rare situation. Generally, the re genetic test is used to verify whether the original driver gene is wrong or incomplete. Therefore, if it is blood test, it is better to stop the drug for a few days; If it is a tissue test, it is the same as secondary drug resistance. It is OK to consider whether to stop the drug according to the side effects of the drug.
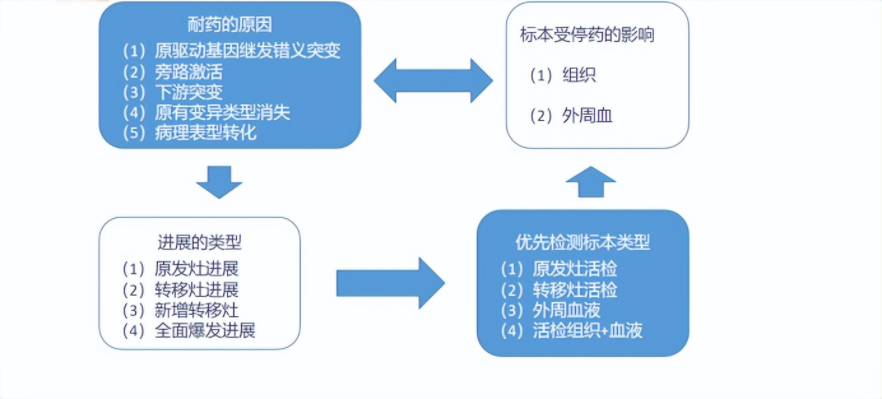
The above figure shows a series of problems that need to be considered when discussing whether to stop drug resistance and retest after drug resistance. Today, we will focus on the causes of drug resistance and the impact of drug withdrawal on the samples.
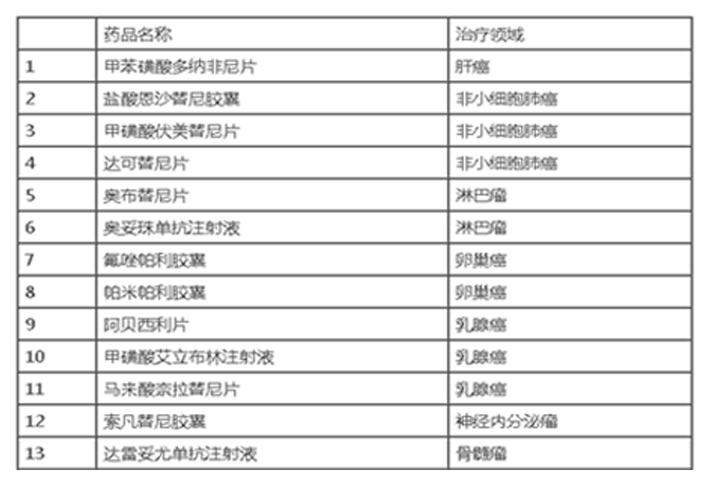
Causes of drug resistance in targeted therapy and corresponding treatment methods
After the targeted treatment of drug resistance, there are clear reasons for drug resistance at the gene level and the corresponding treatment methods, which were discussed in detail in our previous articles.

Possible causes of drug resistance in different types of progression
The progression of primary foci is relatively diverse, among which new drug resistance genes are the most common, that is, secondary variation of the original gene, new bypass activation, and new downstream variation. In addition, phenotypic transformation and disappearance of original driver genes also occurred. What is more embarrassing is that a high proportion of the test results are that the original driver genes are still there, and no typical drug resistance genes are found.
The progression of metastatic foci is relatively simple. After all, most of the metastatic foci are "colonies rapidly developed in a short time" by single cells or gene single cell clusters. The genes are relatively simple and the development time is relatively short. If secondary drug resistance occurs after a period of time, different from the original drug-resistant cell types that may lurk in the primary foci, the drug-resistant genes in the metastatic foci are basically the types that survive unexpectedly under the attack of targeted drugs and in the "stress response" of the cells, that is, the newly increased drug-resistant genes.
The newly confirmed metastatic foci are generally "potentially latent and originally drug-resistant cell types" in the primary foci that "run out to open up colonies" during the treatment process. Only with the original drug resistance gene, new drug resistance gene, no current known typical driver gene, and the phenotype changes to small cells or squamous cell carcinoma can be seen in clinical practice. Therefore, it is particularly important to further detect the targeted biopsy of new metastases.
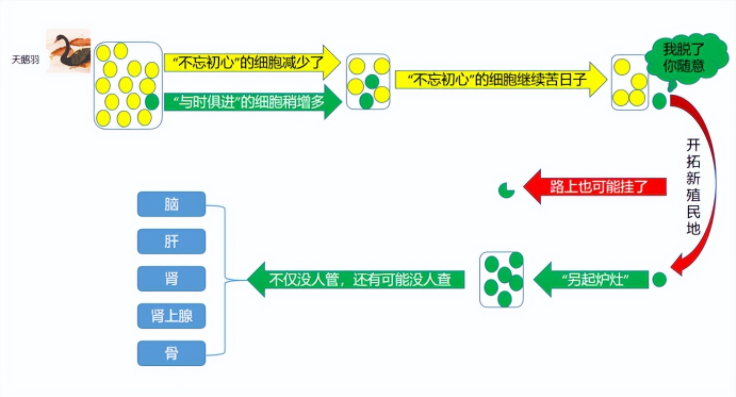
The reasons for the overall outbreak of progress are also relatively simple. If there is no problem with the quality of the drug in hand, it is very unlikely that many of the primary foci, the original metastatic foci and the new metastatic foci will have the same cause of drug resistance, which is often due to two situations: bypass activation in the new drug resistance genes - for example, met amplification and HER-3 overexpression in the secondary drug resistance of EGFR; The human body's own metabolism causes the drug concentration of the targeted drug to drop - this extreme condition is often accompanied by the sudden disappearance of the originally serious drug side effects during the treatment process.
Preferential selection of specimens after targeted treatment of drug resistance
It is often seen on the Internet that the tissue of the test specimen is superior to the pleural effusion and ascites, and the pleural effusion and ascites are superior to the peripheral blood. But in fact, this statement is only the ranking of the gene detection rate in the specimen, which is not consistent with the actual consideration of drug resistance. The purpose of gene testing after drug resistance is to find the cause of drug resistance, strive to solve the problem of treatment within the scope of targeted therapy, and detect the lesions without drug resistance. Even if the results of gene testing of tissues are only the original driver genes can be detected, it is meaningless. As for the new brain parenchymal metastases that have not progressed in other locations, the primary lesions can not be touched no matter how easy the biopsy is - if there is no way to perform brain surgery, blood is the only reasonable specimen selection.
To add a special case in the association between the selection of specimens and the cause of drug resistance, the common pleural metastasis progression (or accompanied by increased pleural fluid) in advanced lung cancer is often encountered in clinical pleural biopsy or pleural fluid detection, which shows that it is still the original variant type. The reason for drug resistance in this situation is that local metastases do not depend on blood supply but are nourished by pleural fluid, and the concentration of targeted drugs in pleural fluid is too low. Therefore, the conventional treatment is thoracic perfusion therapy (chemotherapy drugs or anti vascular drugs), rather than re examining and looking for drug resistance genes.
Samples for genetic testing were affected by drug withdrawal
Tissue testing: since it is necessary to confirm the tumor acquisition through pathological results before considering gene testing after biopsy, the success rate of tissue biopsy and gene testing are mainly affected by pathological operation, and drug withdrawal has little effect on the change of tissue level.
Genetic detection of pleural effusion: it may be an advantageous option to extract pleural effusion at the time of diagnosis when the lung lesions are not convenient for biopsy. However, the previous analysis has shown that pleural effusion is often not helpful in drug resistance.
With the improvement of gene detection technology, MRD (tumor micro residue, i.e. quantitative detection of target driver genes by peripheral blood circulation DNA detection technology) used to quantitatively find driver genes in blood has become a new favorite of scientific research. At present, there are two widely recognized conclusions: comparing MRD before targeted therapy and one month after targeted therapy, if it is significantly decreased, it indicates that the effective period of targeted therapy may be longer; When the target treatment reaches the point where the focus can not be seen on the image, the MRD is evaluated. If it is lower than a certain set value, the target drug can be suspended (called "drug holiday"), and the MRD is regularly detected. When the MRD rises above the set value, the original target treatment can be restarted. From these two cutting-edge applications of MRD, we can also learn two points:
(1) The use of targeted therapy can reduce the amount of free DNA in blood, so that it is lower than the detectable range of technology in genetic testing. Then, should this be considered in drug resistance? When the targeted therapy is effective, the amount of free DNA in the blood of controllable gene variation types is reduced, while the secondary drug resistance is due to the occurrence of uncontrollable gene variation types, so drug withdrawal will not lead to the increase of uncontrollable free DNA; However, it will lead to an increase in the types that can be controlled, and the amount of free DNA of uncontrollable types will not be affected without stopping the drug, so there is no need to stop the drug.
(2) After drug withdrawal, the amount of free DNA in blood will be increased. However, in addition to the amount of free DNA that can drive gene types, there is also a problem of time. The regular detection MRD in the "drug holiday" is measured in months. However, the drug withdrawal period before the genetic test discussed now is usually only a few days, and this gap is still quite large. Even in order to see the change of the original variant type, The withdrawal of drugs for several days is obviously a drop in the bucket to increase the amount of free DNA, so there is no need to wait, and it can be tested as soon as possible.
When it comes to increasing the amount of free DNA in blood, especially the amount of drug-resistant genes, it may be more possible to "capture" drug-resistant variant genes by performing blood gene testing during local radiotherapy after drug resistance. It is hoped that there will be research in this field in the future.
After secondary drug resistance, do you need to stop the targeted drugs before genetic testing?
Since tissue testing, pleural fluid testing and blood testing will not have any beneficial impact on the re genetic testing just because the targeted drug is stopped for a few days, instead, it will delay the time to obtain the test results as soon as possible. Therefore, we only need to stop the drug for a certain time when the side effects of the targeted drug interfere with the biopsy.
Source:
https://www.cn-healthcare.com/articlewm/20220817/content-1419772.html