Cancer has become the second leading cause of death in the world. According to the heavy data released by the Lancet a few days ago, drinking has become the top two major cancer risk factors after smoking [1]. As many as seven cancers have been explicitly listed as "alcohol related cancers". In 2020 alone, the number of new cancer cases caused by alcohol consumption in the world will exceed 740000 [2].
Although it is a consensus that drinking can cause cancer, why is everyone's motivation to quit drinking far less than to quit smoking? One reason is that there are few studies on changes in alcohol consumption, including increase, decrease and abstinence.
In addition, there are different people (species) involved in alcohol metabolism. Maybe they are the "sons of God" who can drink!
Recently, the JAMA sub journal published Association Between Changes in Alcohol Consumption and Cancer Risk, which analyzed the relationship between changes in alcohol consumption and the risk of alcohol related cancer and the occurrence of all types of cancer on the basis of three consecutive health examination data of more than 4.5 million Koreans [3]. Today, we will talk about drinking, abstinence and cancer based on the latest and previous research~
"Seven Heavenly Kings" of Alcohol related Cancer
In 2021, The Lancet Oncology released the Global budget of cancer in 2020 attributable to alcohol consumption: a population based study, which specifically analyzed the global cancer burden caused by alcohol. The results showed that in 2020, there were about 740000 new cancers worldwide that had a causal relationship with alcohol consumption.
The types of cancer with the largest number of new cases related to alcohol consumption in 2020 include:
1. Esophageal cancer (189000 cases)
2. Liver cancer (154700 cases)
3. Breast cancer (98300)
4. Colon cancer (91500)
5. Rectal cancer (65100)
6. Oropharyngeal carcinoma (39400)
7. Laryngeal cancer (27600)
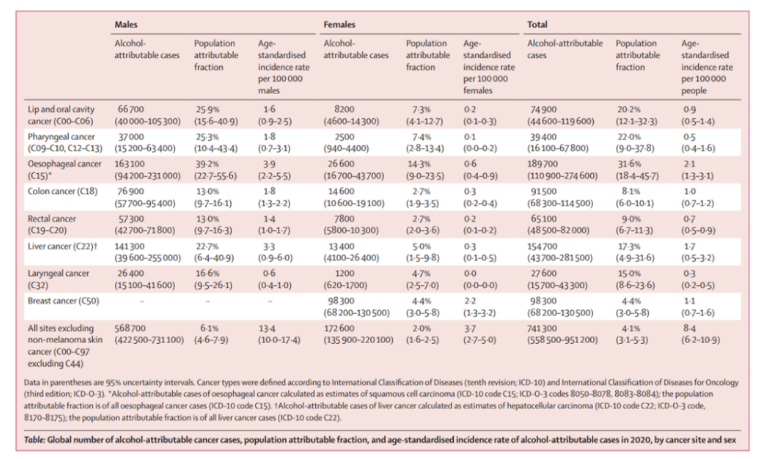
Number of global alcohol related cancer cases, population proportion and age standardized incidence rate by cancer location and sex in 2020
It is worth noting that the risk of alcohol related cancer in East Asia, including China, is higher than that in other regions: the regions with the highest proportion of cancer cases attributable to alcohol are East Asia (5.7%) and Central and Eastern Europe (5.6%), while North Africa (0.3%) and West Asia (0.7%) have the lowest proportion.
Researchers predict that with the economic development, the alcohol consumption in China, India and other countries will also increase, which is "icing on the cake" for alcohol related cancer data.
In a study published in British Journal of Cancer in 2020, 226162 Australian participants ≥ 45 years old (2006-2009) were analyzed for cancer risk adjusted risk ratio (HR) related to total alcohol intake (drinking/week) [4].
During a median follow-up period of 5.4 years, 17332 cancer cases were diagnosed. Different amounts of alcohol consumption lead to different degrees of increase in the risk of alcohol related cancer: the liver bears the brunt, and the risk of liver cancer of heavy drinkers who drink more than 28 cups of alcohol per week is 3 times higher than that of light drinkers who drink 1-3.5 cups of alcohol per week (10 g of alcohol per cup); Esophagus follows closely and cancer risk easily doubles. It should be noted that the reference here is "light drinkers" rather than "non drinkers".
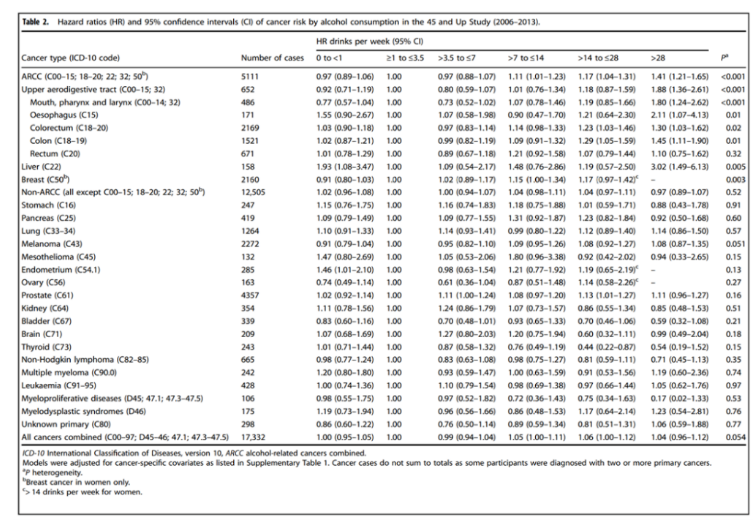
HR of drinking carcinogenic risk, 2006-2013
Drunkard ecstasy: Does abstinence not prevent cancer, or even increase the risk?
To get to the point, the research published by JAMA sub journal this time included participants who were ≥ 40 years old in the Korean National Health Insurance Service, who had undergone health screening in 2009 and 2011 and had recorded drinking status data. The pure East Asian ethnic data may be more worthy of our reference.
Participants were divided into:
No drinking (0 g/d), light drinking (<15 g/d), moderate drinking (15-29.9 g/d) and heavy drinking (≥ 30 g/d);
Then, according to the change of drinking level from 2009 to 2011, it is divided into:
No drinking group, maintain drinking group, increase drinking group, quit drinking group and reduce drinking group.
The primary end point was newly diagnosed alcohol related cancer, including head and neck cancer (oral cancer and throat cancer), esophageal cancer, colorectal cancer, liver cancer, laryngeal cancer and female breast cancer, and the secondary end point was all newly diagnosed cancers (except thyroid cancer).
The final 4513746 participants included in the study, with an average (SD) age of 53.6 (9.6) years, of which 2324172 were male (51.5%). During the median (IQR) follow-up period of 6.4 (6.1-6.6) years, 215676 cancer events (7.7/1000 person years) occurred, of which 37.2% (80263 cases) were alcohol related cancers.
First, there is no doubt that increased alcohol consumption is associated with increased risk of alcohol related cancers and all cancers. There is also a dose response relationship in alcohol related cancer: when never drinking alcohol becomes mild [adjusted risk ratio (aHR), 1.03; 95% CI, 1.00-1.06], moderate (aHR, 1.10; 95% CI, 1.02-1.18) or severe (aHR, 1.34; 95% CI, 1.23-1.45), the risk of alcohol related cancer increases.
Similarly, compared with continuous light drinkers, the incidence of alcohol related cancer increased when drinking from mild to moderate (aHR, 1.10; 95% CI, 1.05-1.15) or severe (aHR, 1.17; 95% CI, 1.09-1.25).

Association between changes in drinking levels and cancer
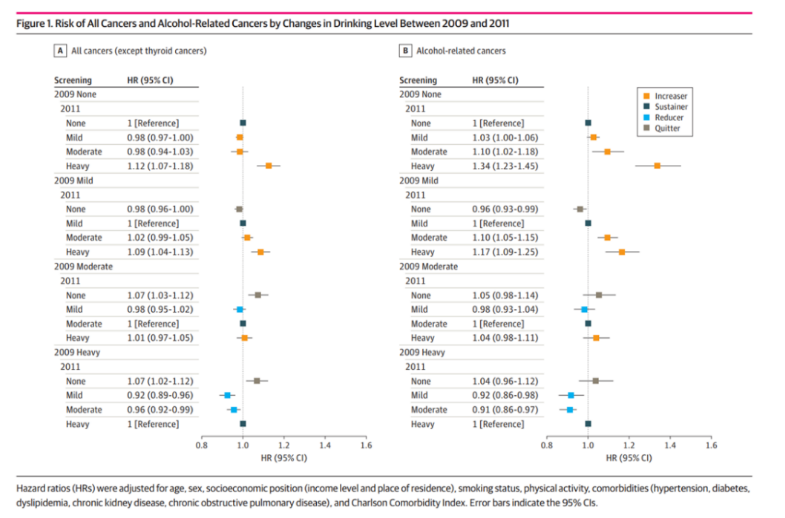
Risk of all cancers and alcohol related cancers caused by changes in drinking levels between 2009 and 2011
This model also applies to all cancers: the increased risk is not only related to the change from non drinking to heavy drinking (aHR, 1.12; 95% CI, 1.07-1.18), but also to the change from light drinking to heavy drinking (aHR, 1.09; 95% CI, 1.04-1.13). The incidence of gastric cancer, liver cancer, gallbladder cancer, lung cancer, multiple myeloma and leukemia is very high if the non drinkers increase their drinking.
However, when it comes to changes in risk of the alcohol related cancer and all cancers caused by abstinence or reduction of the alcohol consumption, it means "unexpected" and "reasonable".
Heavy drinkers who cut back on alcohol consumption had a higher risk of alcohol related cancer than moderate or mild drinkers. The risk of alcohol related cancers (aHR, 0.91; 95% CI, 0.86-0.97) and all cancers (aHR, 0.96; 95% CI, 0.92-0.99) was reduced by changing the amount of alcohol consumed from severe to moderate, and vice versa (alcohol related cancers: aHR, 0.92; 95% CI, 0.86-0.98; all cancers: aHR, 0.92; 95% CI, 0.89-0.96). For the cancer site, the risk of breast cancer, renal cancer and gallbladder cancer in the heavy to moderate drinkers is lower than that in the continuous heavy drinkers.
However, when moderate or severe drinkers begin to abstain from alcohol (compared with those who maintain the same level of alcohol consumption), not only does the risk of alcohol related cancer not change significantly, but the risk of all types of cancer also increases slightly (moderate: aHR, 1.07; 95% CI, 1.03-1.12; severe aHR, 1.07; 95% CI, 1.02-1.12).
See here, are alcohol lovers ready to forward this article to your relatives, friends and doctors who advise you to quit drinking?
However, the second analysis can immediately make the alcoholics "disillusioned". The researchers also conducted three consecutive health screening and drinking behavior analysis on the participants with available data, and found that the increased risk of alcohol related cancer and all types of cancer disappeared for the participants who abstained from drinking during the screening in 2011 and insisted on the screening in 2013.
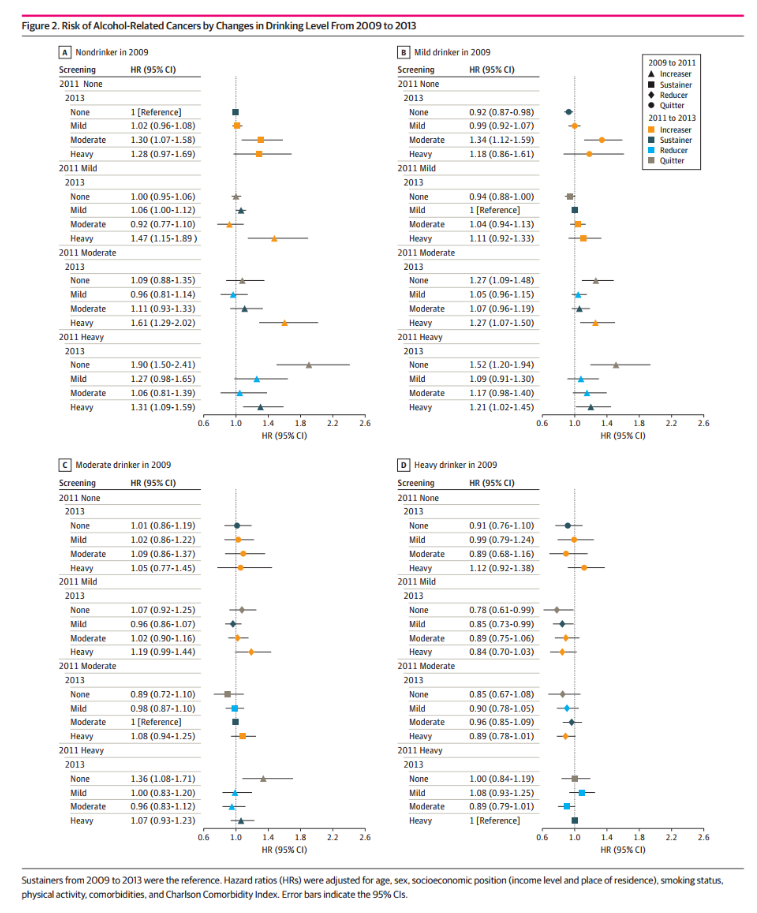
Risk of alcohol related cancer due to changes in drinking levels from 2009 to 2013
The participants who reduced alcohol consumption also benefited significantly. In the screening in 2011, the incidence of alcohol related cancer (aHR, 0.85; 95% CI, 0.73-0.99) and all cancers (aHR, 0.89; 95% CI, 0.81-0.98) were even lower among those whose alcohol consumption was significantly reduced from severe to mild and maintained at the level of light alcohol consumption. Therefore, reducing alcohol consumption is, to some extent, "the harder you work, the luckier you will be".
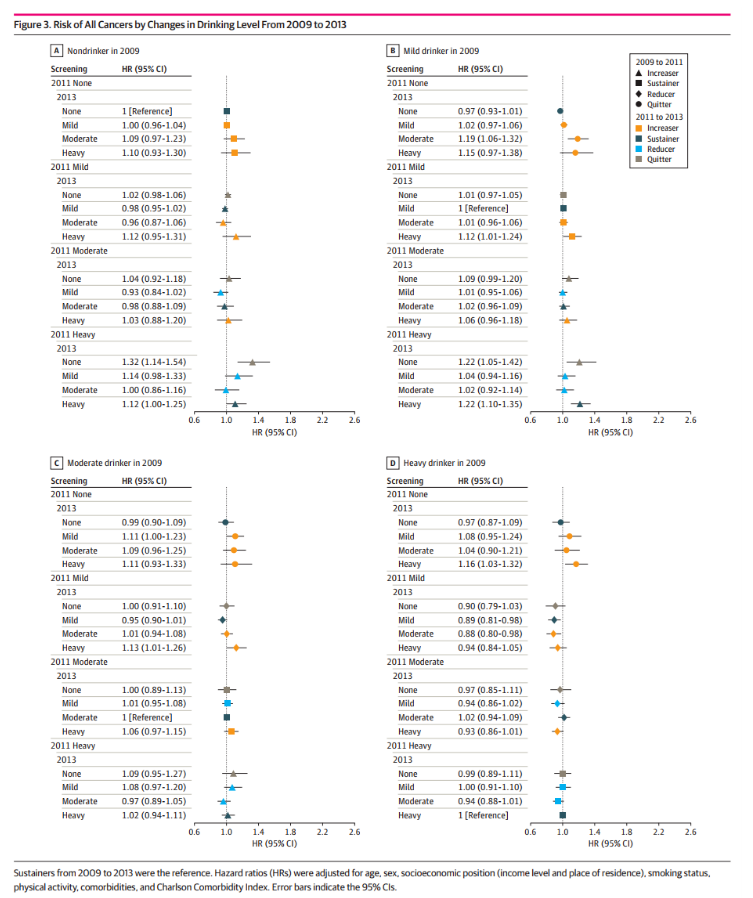
All cancer risks due to changes in drinking levels from 2009 to 2013
In the hierarchical analysis based on age, gender and smoking status, the researchers drew a "focus range": among older, male and never smoking participants, the change in alcohol consumption is more prominent in relation to alcohol and the relationship between the whole cancer species. For example, the aHR of alcohol related cancer in people who did not drink alcohol to become heavy drinkers was 1.70 (95% CI, 1.48-1.94) vs 1.34 (95% CI, 1.20-1.50) for those who were ≥ 65 vs<65 years old, 1.47 (95% CI, 1.35-1.60) vs 0.83 (95% CI, 0.60-1.16) for men vs women, and 1.77 (95% CI, 1.51-2.08) vs 1.49 (95% CI, 1.27-1.75) for current smokers who did not smoke vs ≥ 20 pack years.
It's better to abstain from drinking less than to drink more or make it worse, but the best thing is
A survey of the three studies shows that China and men are the key "victims" of alcohol related cancer. In the report released by The Lancet Oncology, China ranks among the regions with the highest risk of cancer caused by drinking, and the male PAF is significantly higher.
The researchers believe that this is due to the higher frequency of the aldehyde dehydrogenase mutation allele (ALDH2 * 2) (estimated to be 28% - 45%) in East Asian people. After drinking, the acetaldehyde metabolism of these people slows down and accumulates in the body, resulting in blushing, nausea, vomiting, sweating, palpitations and other adverse reactions, which is what we call "drinking on the face". People who are "good at drinking" should usually drink less or no alcohol, but the reality is that they will drink right.
For cancer, there is no such thing as "a small drink is good for you, but a big drink is bad for you". Previous studies have shown that even a small amount of alcohol consumption increases the risk of cancer, including most upper gastrointestinal cancers and gastrointestinal cancers. Existing research continues to emphasize that there is no safe level of drinking in terms of cancer risk.
As for the "abstinence cannot change or even slightly increase the risk of cancer" that makes alcohol lovers feel lucky, or the bias of "pathological abstinence" - people may stop drinking when they feel symptoms and/or other adverse health effects. This phenomenon disappeared after a longer follow-up time: in the subgroup analysis of the three evaluators, those who abstained before the screening in 2011 and remained non drinkers during the screening in 2013 could see a significant reduction in risk. Therefore, abstinence should not only be started as early as possible, but also be persisted for a long time.
In addition to being long enough, it is also crucial to reduce the amount of alcohol consumption sufficiently: both the increase and decrease of alcohol consumption have a significant dose-response relationship with cancer risk. However, no matter how the drinkers reduce or even quit, the losses caused are irretrievable - they are still at a higher risk of cancer than those who remain sober. Therefore, it is the best choice to never hold up a glass of wine rather than reduce drinking and give up drinking.
Reference
[1]GBD 2019 Cancer Risk Factors Collaborators. The global burden of cancer attributable to risk factors,2010-19:a systematic analysis for the Global Burden of Disease Study 2019.Lancet. 2022 Aug 20; 400(10352):563-591.doi:10.1016/S0140-6736(22)01438-6.PMID:35988567.
[2]Harriet Rumgay,Kevin Shield et al.Global burden of cancer in 2020 attributable to alcohol consumption:a population-based study. Lancet Oncol. 2021 July.
[3]Yoo JE,Han K,Shin DW,et al.Association Between Changes in Alcohol Consumption and Cancer Risk[J]. JAMA Netw Open. 2022 Aug 1; 5(8):e2228544.doi:10.1001/jamanetworkopen.2022.28544.
[4]Peter Sarich. et al.Alcohol consumption,drinking patterns and cancer incidence in an Australian cohort of 226,162 participants aged 45 years and over. British Journal of Cancer.2020.
Source link:
https://www.cn-healthcare.com/article/20221009/content-573738.html